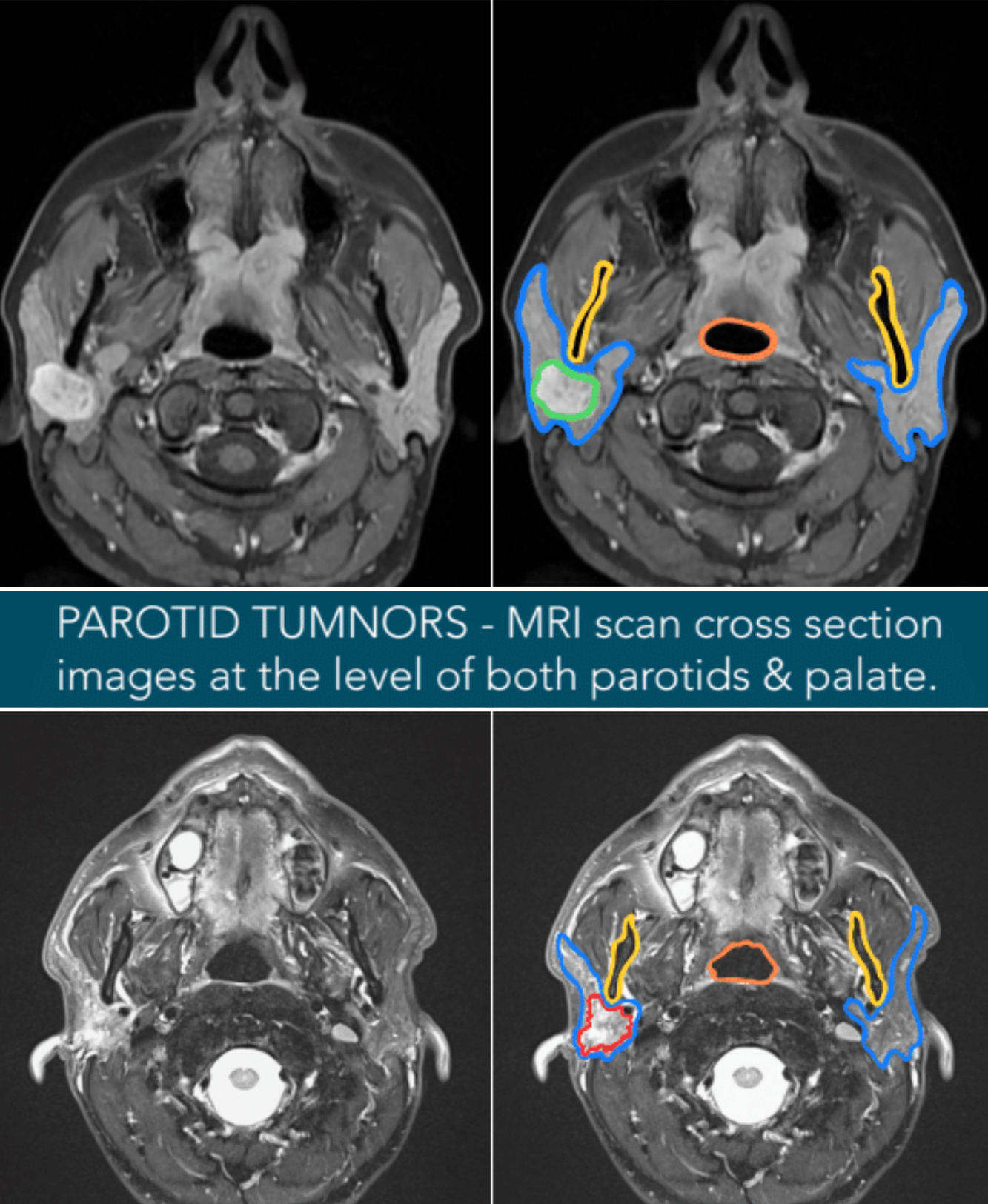
MRI is a very sophisticated scan that shows the parotid gland itself in detail, along with the dimensions and shape of a tumor. It also shows other soft tissue structures such as muscles, fat, blood vessels, lymph nodes, and the spinal cord in great detail. It uses magnets to create the image, meaning there is no radiation exposure. It is very useful in showing the characteristics of the tumor that may indicate it has features that are suspicious for cancer and how to best approach tumors that are deeper in the parotid gland for a needle biopsy.
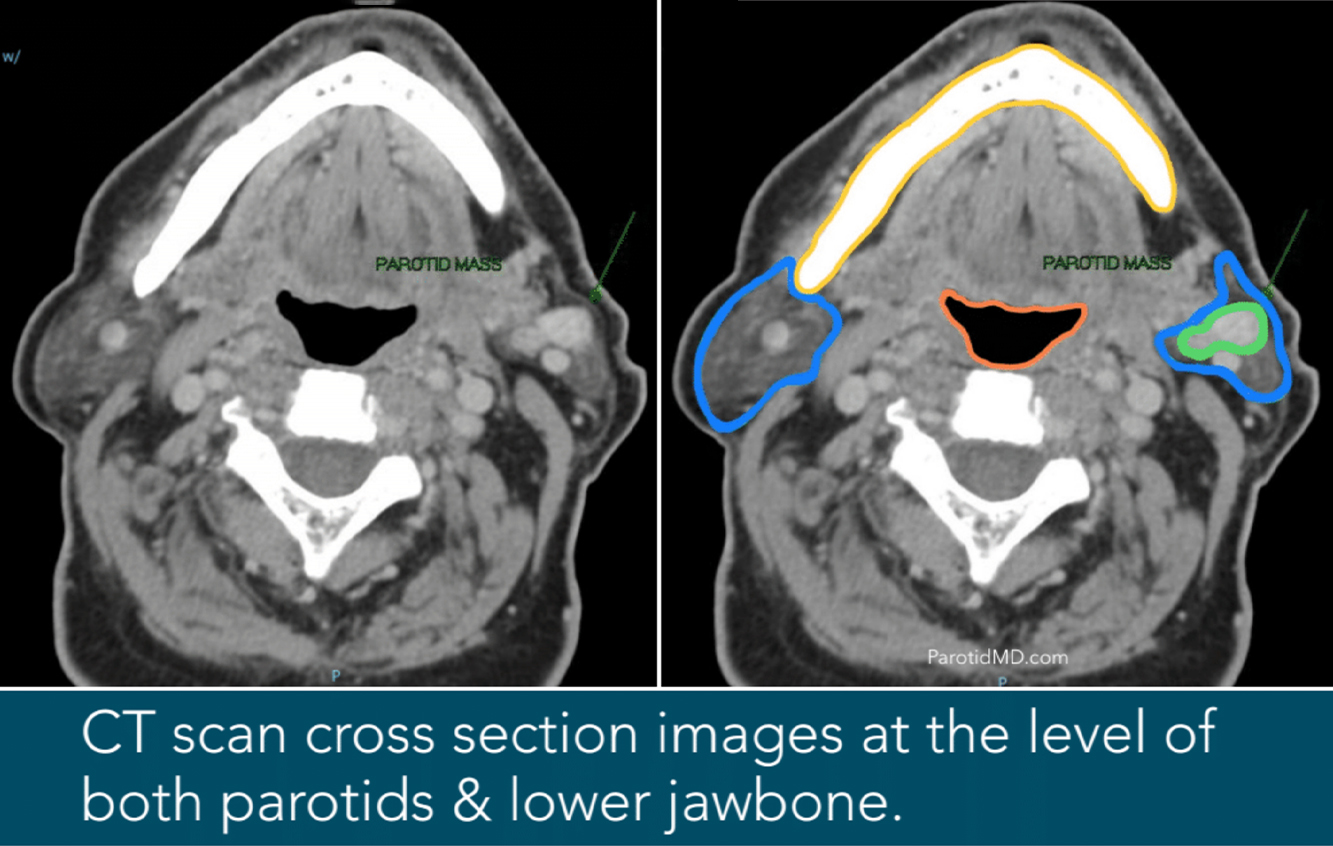
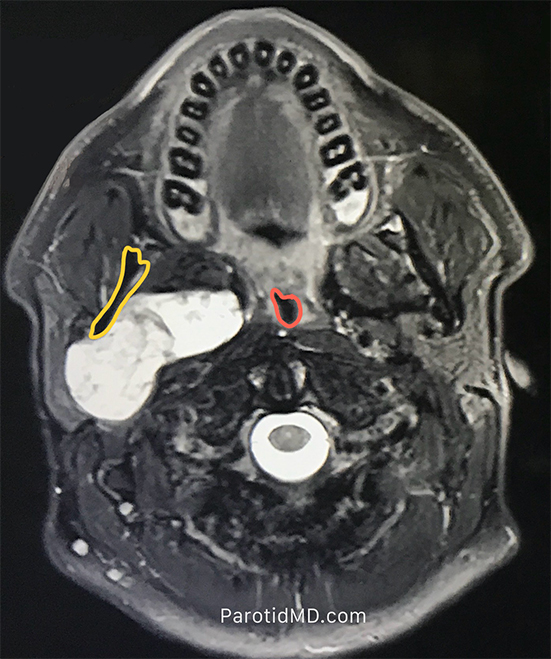
PAROTID TUMOR – In the images on the right, you can clearly see the anatomy with both parotids outlined in blue, the top portion of the jawbone just in front of it in yellow, and the throat outlined in orange. In the top set of images, the tumor is bright white (outlined in green) with smooth borders, extending from the superficial to the deep aspect of the parotid behind the jawbone. It is impossible from these images to tell if this is a cancerous or benign tumor, but it is clear that the tumor is distinct and not invading the surrounding tissues (bone or muscle).
The bottom images show a tumor whose borders are not distinct at all; It is hard to tell where it begins or ends; a rough outline is drawn in red, but there is a possibility that the tumor is invading the muscles behind it. This lack of distinct borders is very suspicious for a cancerous process. The areas of the lymph nodes in the neck can also be examined to see if there are any enlarged, suspicious lymph nodes. This allows the surgeon to plan the optimal surgical strategy and determine what type of reconstruction should be done.
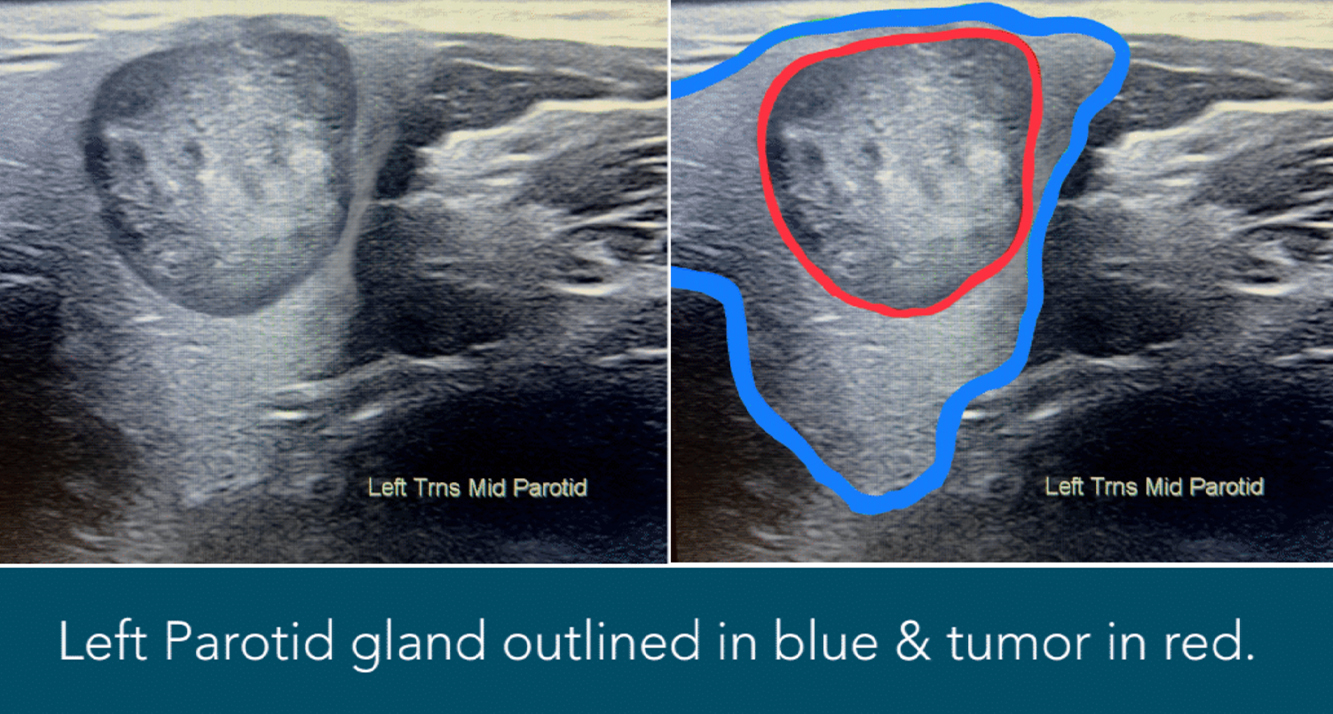
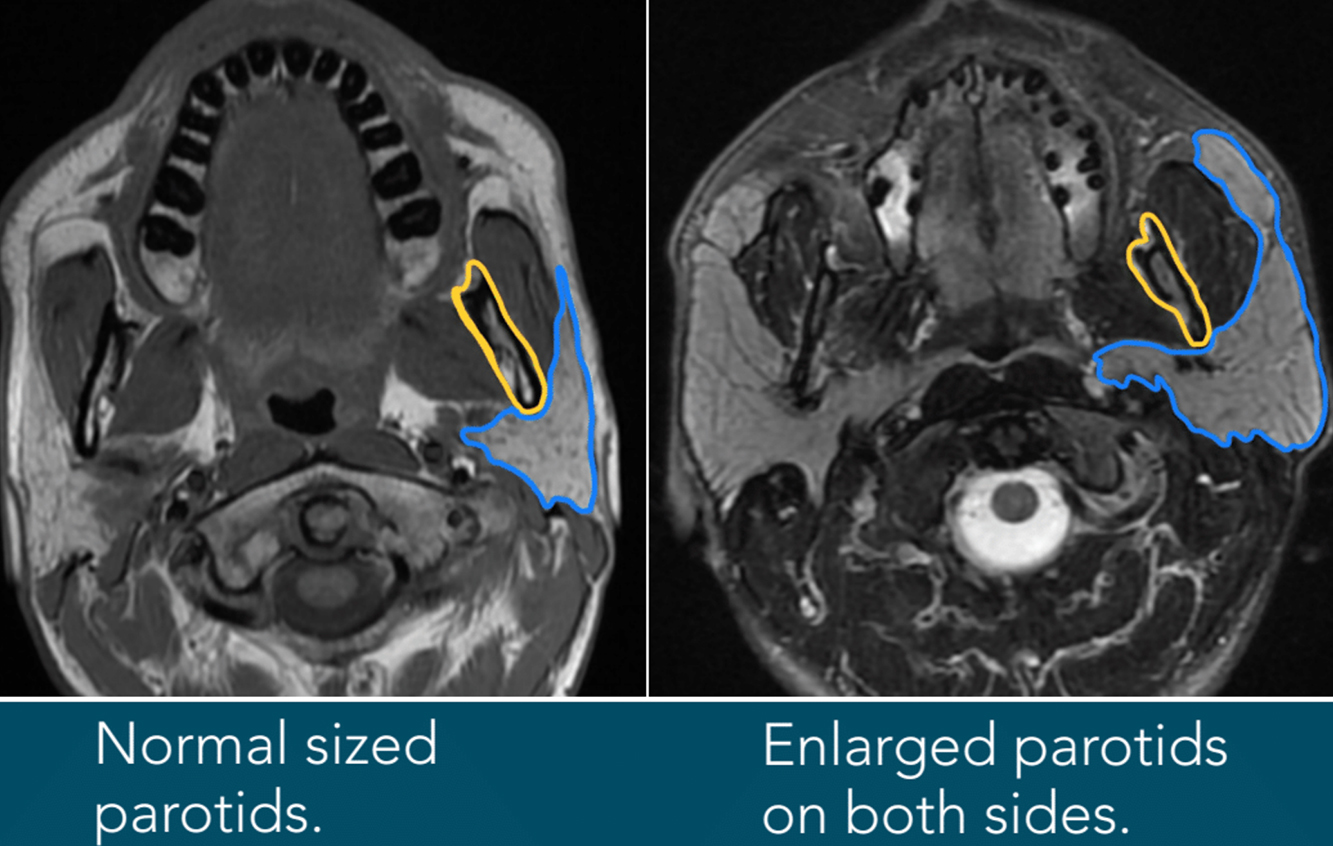
PAROTID ENLARGEMENT – In the images on the right, you can see the parotid glands well outlined in blue. The normal-sized parotid glands are flat and occupy very little space on the side of the face. The enlarged parotid glands occupy significantly more space. In the case shown here, the parotids are both very enlarged, bulging outward, as well as growing inwards and forward towards the duct.
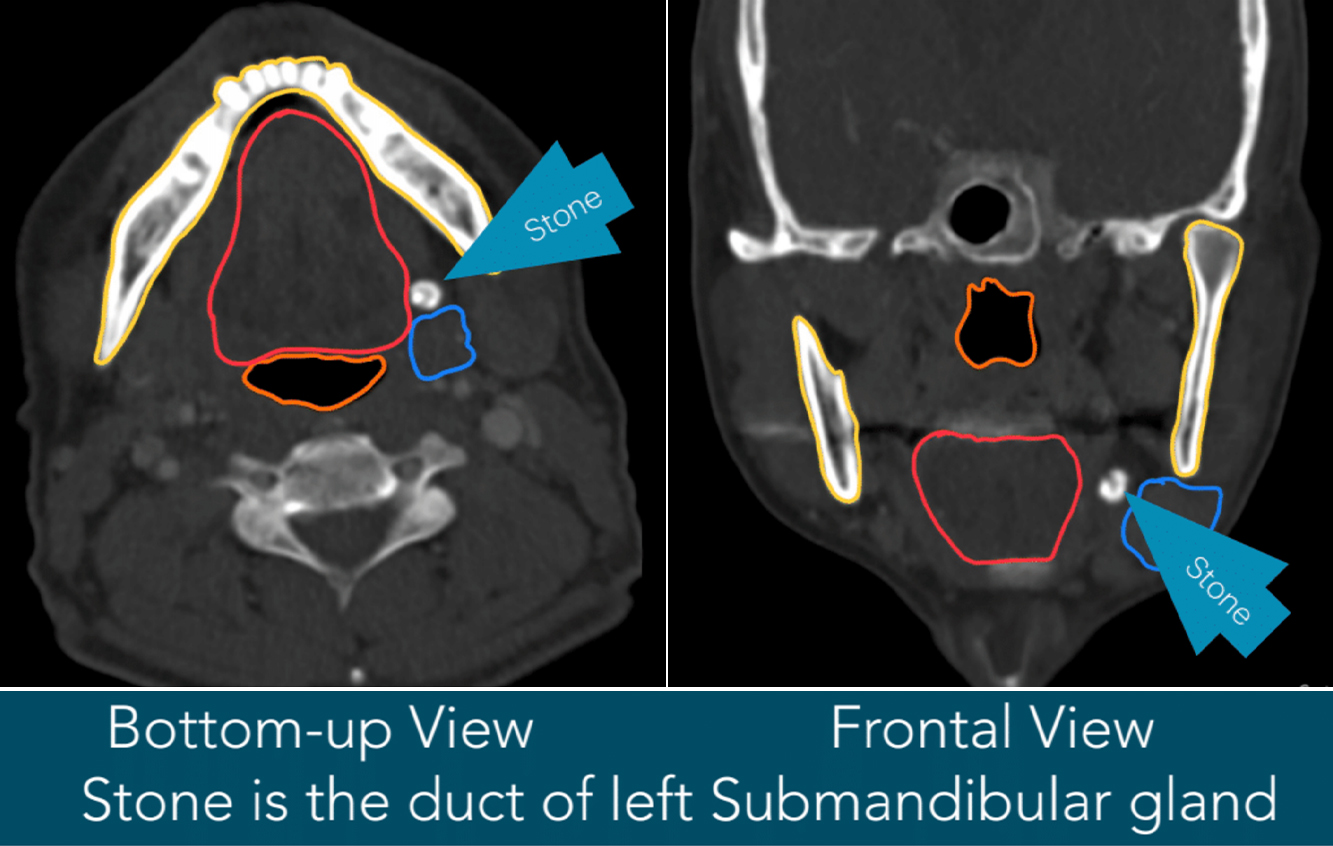
The jawbone, outlined in yellow, shows how much of the parotid gland is growing deeper inwards and towards the throat, while the majority of it is growing outward and bulging against the skin.