Is the facial nerve less visible when performing a micro-parotidectomy? Is the facial nerve at more risk?
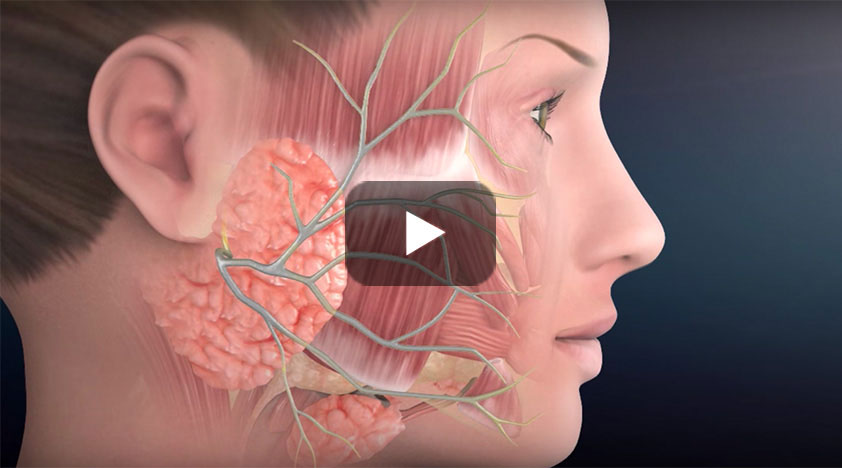
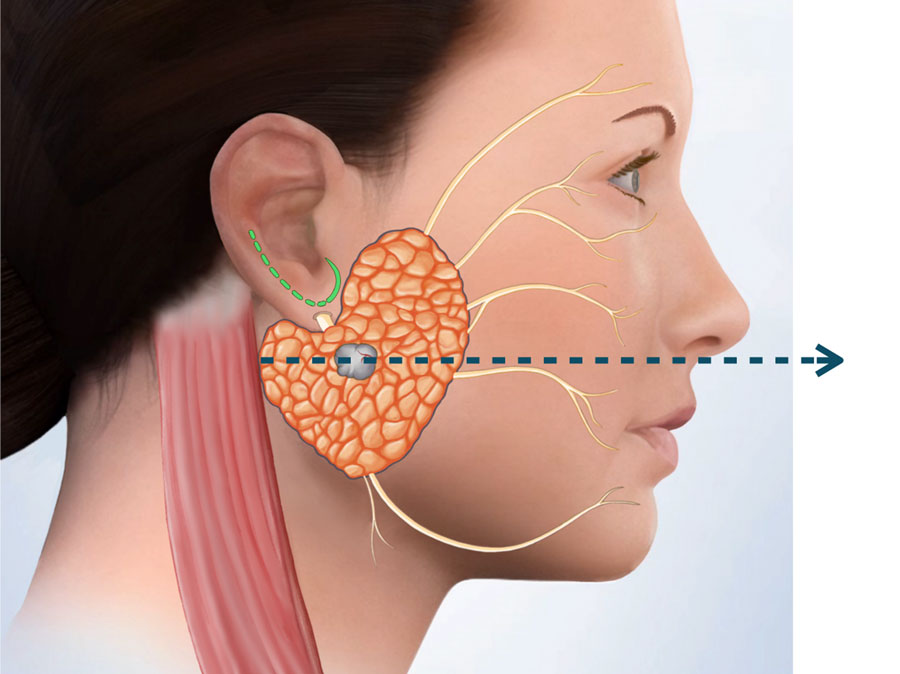
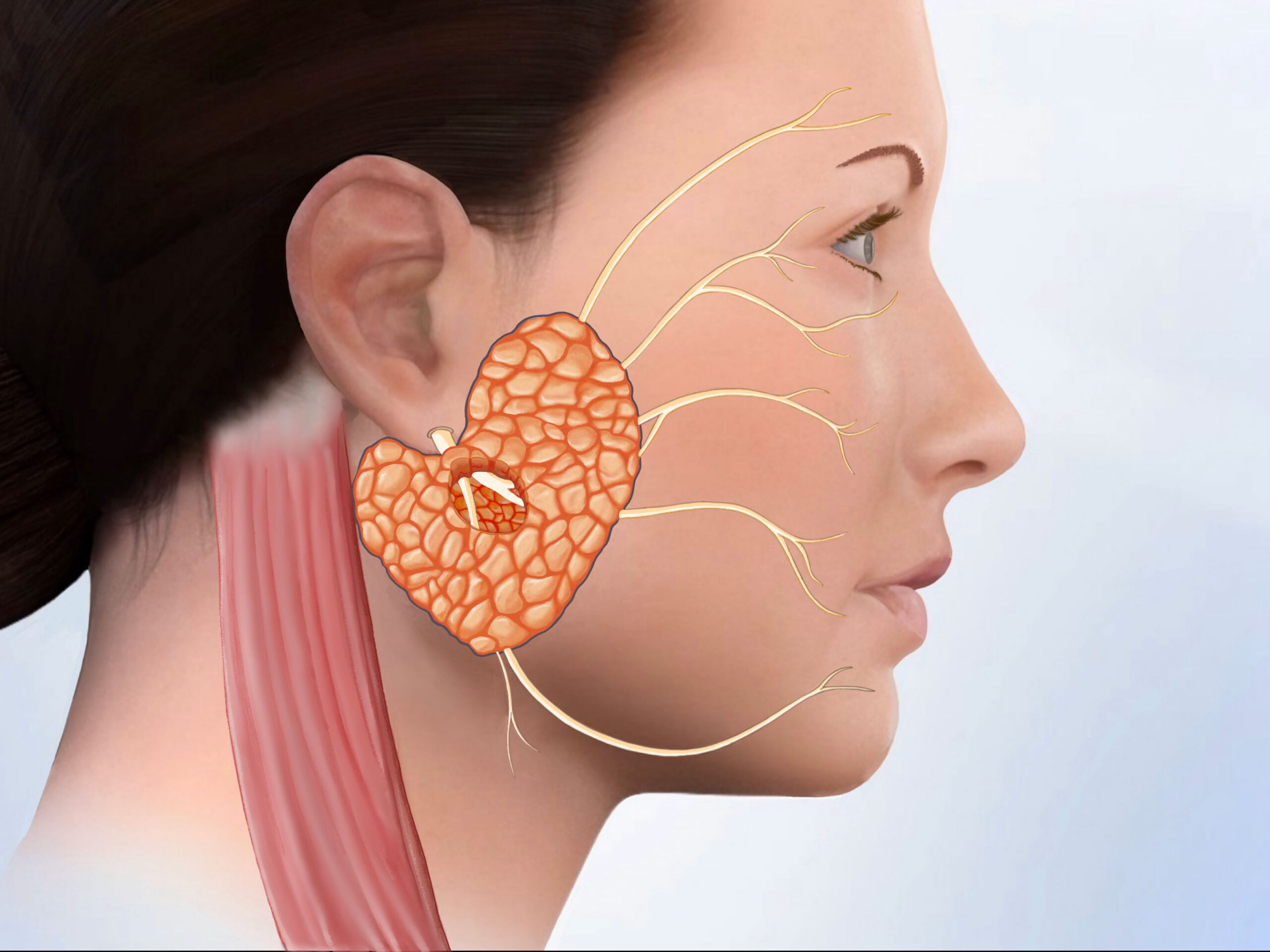
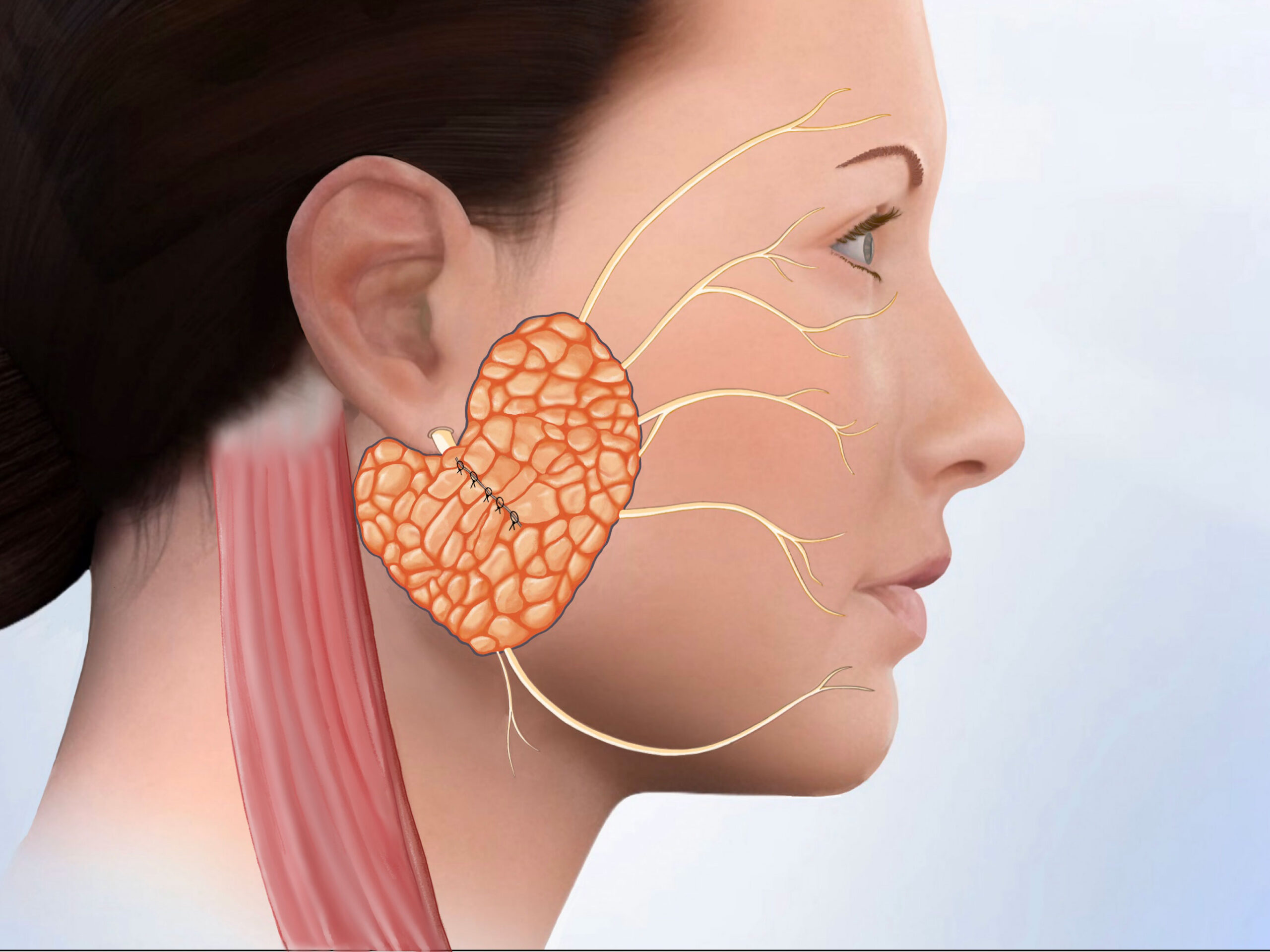
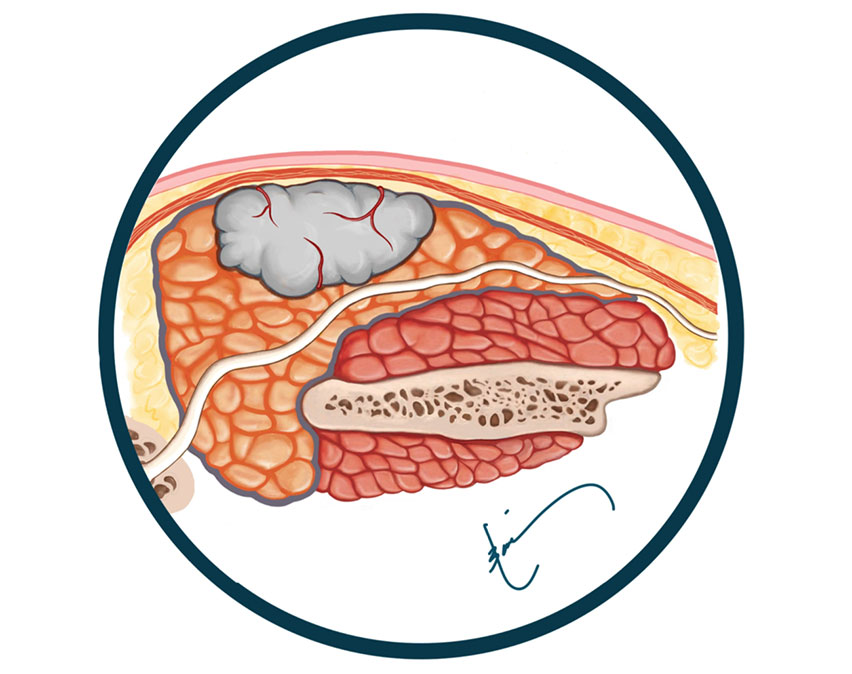
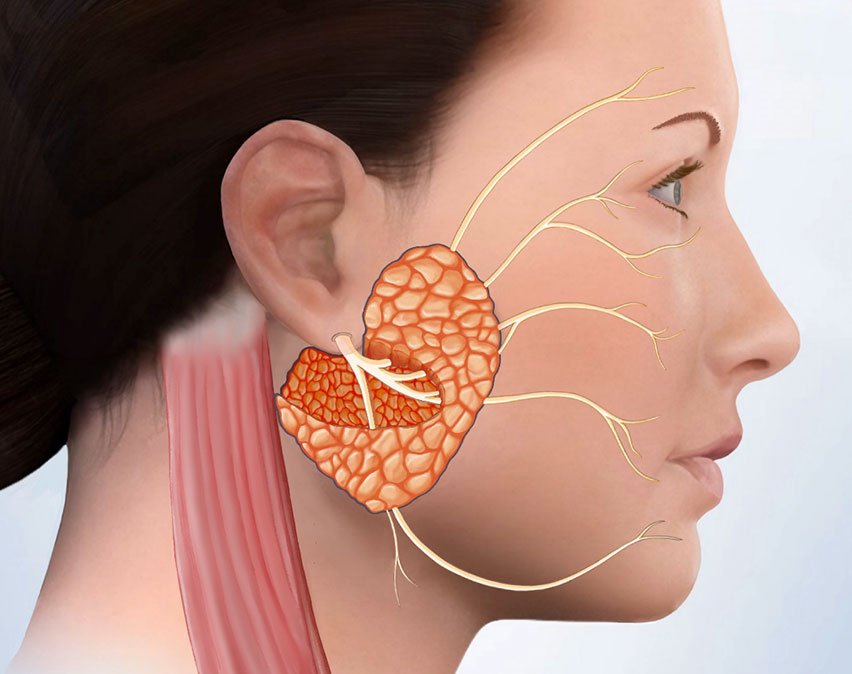
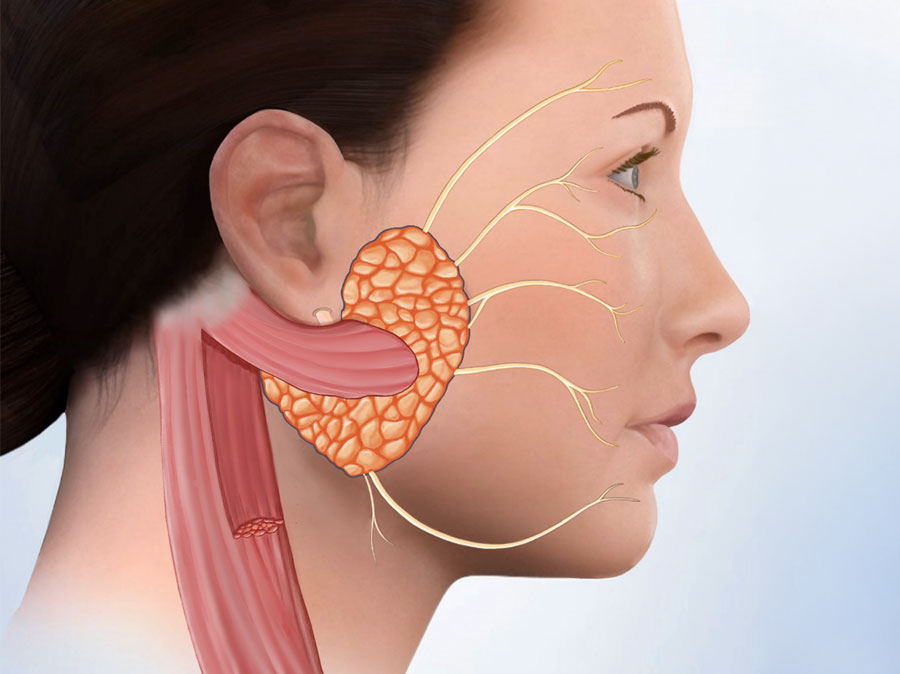
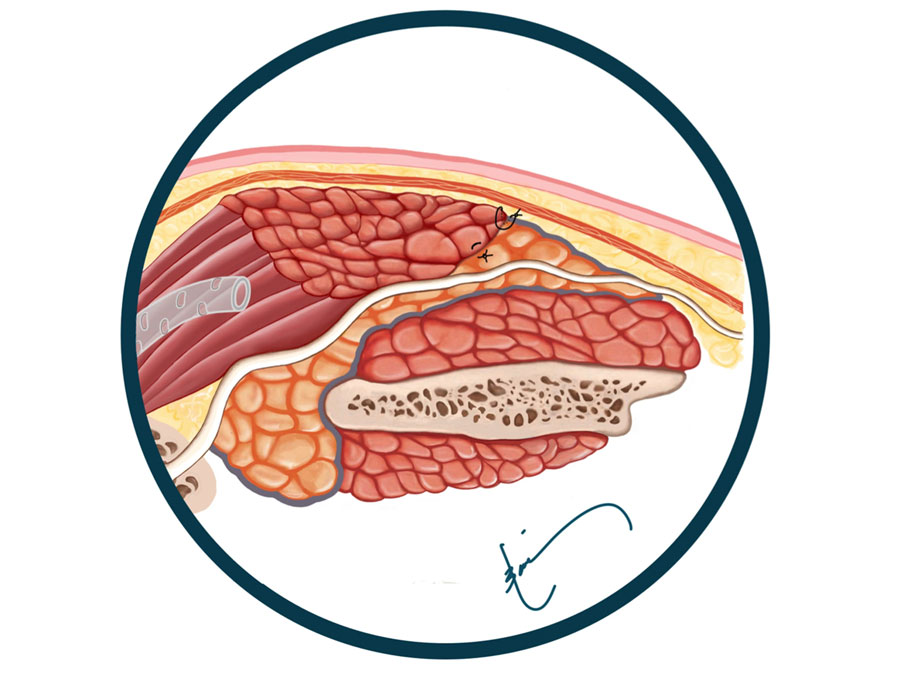
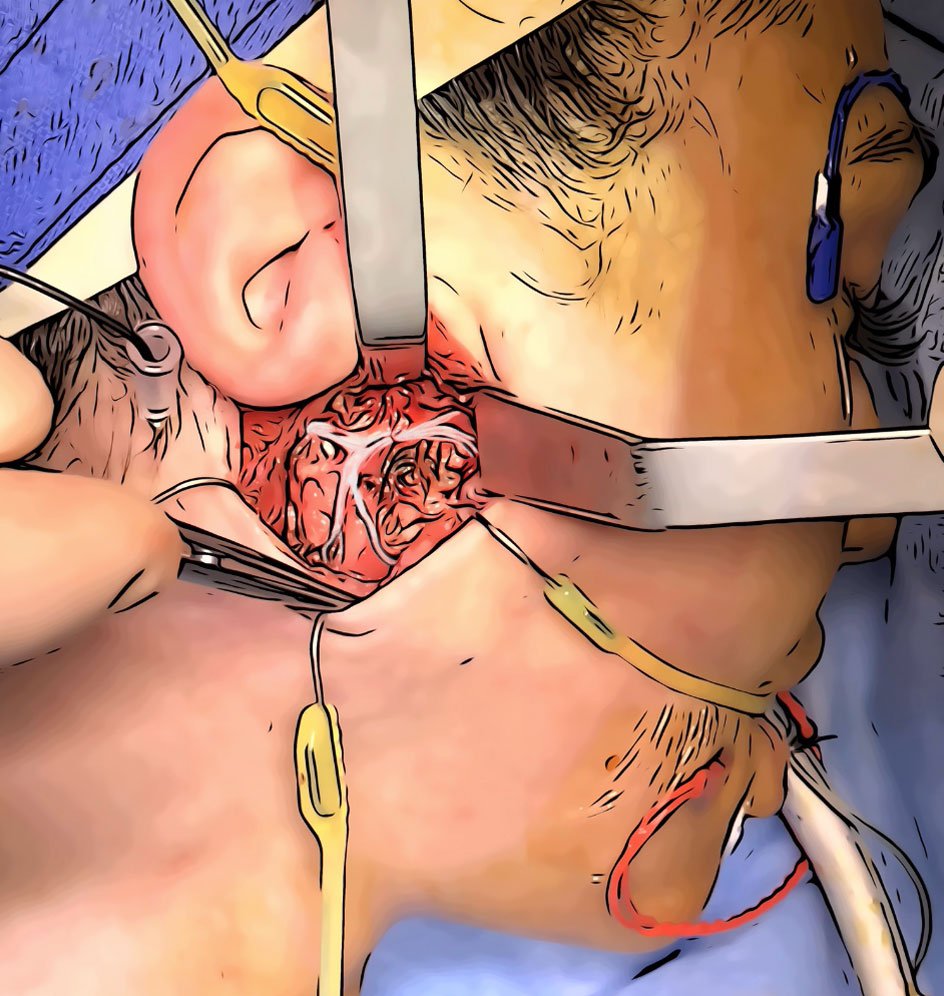
ABSOLUTELY NOT. Micro-parotidectomy is just as safe as any other approach to the parotid gland. As you can see from the image to the left, the entire facial nerve anatomy in the parotid is visible during a micro-parotidectomy. The facial nerve is too important to ever be compromised. The key to preserving the facial nerve is to be meticulous, attentive, gentle, and very patient. This is not a surgery to be rushed; rather, your surgeon needs to be very experienced, caring, and measured.
At the CENTER, we not only treat parotid tumors but also cases of facial paralysis caused during surgery by other surgeons; as such, we have an immense respect for the facial nerve, and we really understand its importance.
In our experience at the CENTER, the incidence of facial nerve issues during micro-parotidectomy has been significantly less than 1%. Even the incidence of temporary weakness has been exceedingly low because we take our time and handle the tissue very gently.